As the name suggests, non-barrier contraceptive methods do
not cause a physical barrier between sexual partners. Therefore it is important
to highlight that these methods do not
protect the user from sexually transmitted diseases. These methods are for the prevention of pregnancy. Fertility-based contraception is not discussed in this post.
The following
information is not intended to replace consultation with a qualified medical
practitioner. If you wish to make an informed decision about the contraception
you use please make an appointment with your local GP or family planning
services.
Emergency contraceptive
pill 1,2
-
Known as: “the morning after pill”
-
What is it? A tablet used to prevent pregnancy
after sex if there is failure of other methods of birth control or the sex was
unprotected. Examples of contraceptive failure includes:
o
Condom breakage or removal during sex
o
Movement or breakage of cervical cap or
diaphragm
o
Intrauterine device or vaginal ring coming out
o
Failure to take regular birth control pills
-
Options: Hormonal and non-hormonal options
available
-
Efficacy: You can take
them up to 120 hours (5 days) after sex, although the treatment become less effective
as more time goes by
-
Side effects: Most commonly nausea and vomiting
-
The emergency contraceptive pill is available
over the counter in Australia without a prescription.
Contraceptive pills 1,3
-
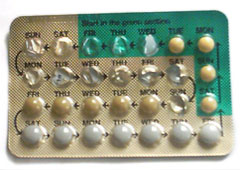
Known as: “the pill”
 |
| An example of a contraceptive pill packet. Image from here. |
-
What is it? A tablet
taken every day containing one or more female hormones used to prevent
pregnancy through:
o
Ovulation prevention
o
Maintaining a thin
lining in the uterus
o
Maintaining viscous
mucus in the cervix to stop sperm
-
Options: There are
many different types of contraceptive pills, some will contain the female
hormones oestrogen and progestin, while others are progestin only.
-
Side effects: Within
the first few months of starting the contraceptive pill it is common to see
nausea, breast tenderness, bloating, mood changes and irregular vaginal
spotting or bleeding.
-
Efficacy: If taken
properly (same time every day with no missed pills) contraceptive pills are
very effective with a failure rate of approximately 0.1%. When the pills are
not taken properly the failure rate is closer to 9%.
Contraceptive
Injection 1,3
 |
| Intramuscular injection. Image from here. |
-
Known
as: “Depo”
-
What
is it? This is an injection, given under the skin or into the muscle of
the buttock or upper arm. It contains the female hormone progestin that
prevents pregnancy by: ovulation prevention and maintaining viscous cervical
mucus to stop sperm migration. Contraceptive action lasts approximately 12
weeks.
-
Side
effects: Within the first 3-6 months irregular or prolonged vaginal
bleeding and spotting are common. After a year approximately 50% of women
completely stop having menstrual periods, however the generally return within 6
months of the last injection.
-
Efficacy:
Contraceptive injection is very effective, with a failure rate of <1%.
 |
| Contraceptive skin patch. Image from here. |
Skin
Patches 1,3
-
What is it? Contraceptive skin patches, work
in a similar way to contraceptive pills. They both contain the female hormones
oestrogen and progestin, which work by: ovulation prevention, maintaining a
thin uterus lining, and maintaining viscous cervical mucus to stop sperm
migration.
When using this method a patch is
worn on the upper arm, shoulder, upper back or hip and is changed weekly.
Patches are worn for 3 weeks followed by a 1 week break in which the menstrual period
occurs.
-
Side effects: The side effects of the patch are similar to those
of a birth control pill (above). There is considered to be a higher risk of
developing a blood clot when using the contraceptive skin patch.
-
Efficacy: The contraceptive skin patch is considered as effective as the contraceptive pill. With a 0.3% efficacy for perfect use and 9% efficacy for typical use.
Vaginal
Ring 1,4
 |
| Vaginal ring positioning. Image from here. |
-
What is
it? A flexible plastic ring that is inserted into the vagina. The contraceptive
vaginal ring contains oestrogen and progestin which is absorbed by the body on
contact. It prevents pregnancy by: ovulation prevention, maintaining
a thin uterus lining, and maintaining viscous cervical mucus to stop sperm
migration.
Similar
to the skin patches, the vaginal ring is worn on a cycle of 3 weeks inside the
vagina followed by 1 week without the ring, in this week the menstrual period
occurs.
-
Side
effects: Once again the side effects of the vaginal ring are similar to
those of birth control pills (noted above).
- Efficacy: Like the contraceptive pill and skin patch, the vaginal ring has an efficacy of 0.3% for perfect use and 9% for typical use.
Contraceptive
Implant 1.5
 |
| Where the contraceptive implant sits. Image from here. |
-
What is
it? A small rod shaped implanted which is inserted into the arm by a
health care worker. They contain progestin which is slowly absorbed into the
body preventing pregnancy by: ovulation prevention and maintaining viscous cervical
mucus to stop sperm migration. Action lasts for up to 3 years.
-
Side
effect: The major side effect associated with the contraceptive implant is irregular
bleeding.
-
Efficacy:
The implant is one of the most effective methods of birth control.
It is effective within 24 hours of insertion.
Intrauterine
devices (IUD) 1,6
-
What is
it? IUDs are plastic devices that release either copper or progestin
and offer long term contraception. They are placed by a healthcare provider
through the vagina and cervix, into the uterus. The mechanism of action is not
fully understood however, it is believed that copper-containing IUDs prevent
fertilisation through sterile inflammatory reaction. While progestin-containing
IUDs, like many of the other contraceptives discussed in this post, prevent
pregnancy by ovulation prevention and maintaining viscous cervical mucus to
stop sperm migration.
 |
| Placing of the IUD. Image from here. |
-
Options: IUDs release either copper or progestin. Depending on the
IUD selected their lifespan can vary from 3-10 years.
-
Side
effect:
o Copper: women may experience longer and
heavier menstrual periods.
o Progestin: some women stop having
menstrual periods when using this method.
-
Efficacy:
IUDs are very effective contraceptives with a pregnancy rate of <1% for both
the copper-containing and progestin-containing IUDs.
References
 Implantable contraceptive devices have been discussed on this blog here. One problem with these devices is that for women who want to come off the devices they must be surgically removed.
Implantable contraceptive devices have been discussed on this blog here. One problem with these devices is that for women who want to come off the devices they must be surgically removed.